


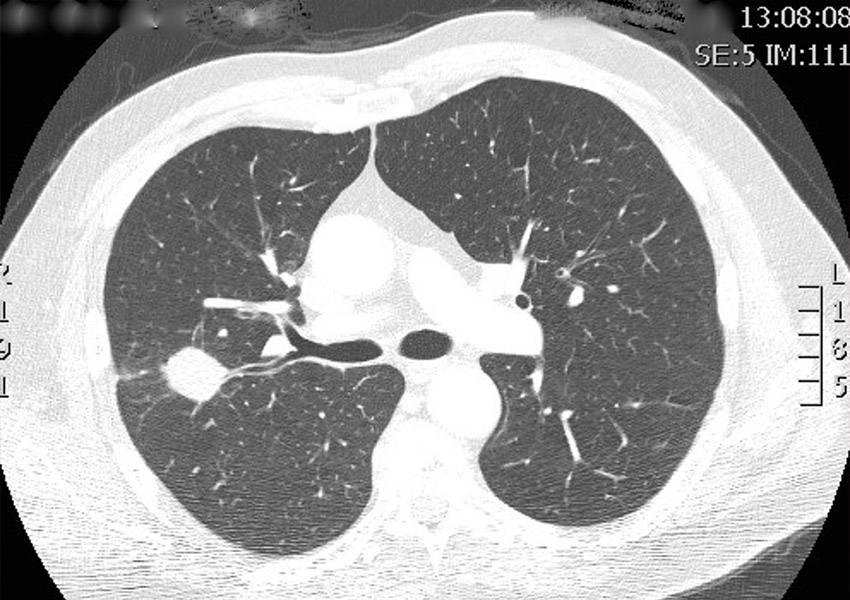
“Your CT scan shows a lung nodule. What happens next?”
It’s a question we hear often. And it’s one that understandably causes anxiety.
With the rollout of Australia’s National Lung Cancer Screening Program, we’re detecting more small lung nodules than ever before. Most of these nodules are benign. But some represent early lung cancer at a stage when cure is absolutely possible.
The challenge isn’t finding nodules anymore.
The challenge is reaching them safely and getting a diagnosis quickly.
That’s where Robotic Bronchoscopy changes everything.
Why early diagnosis matters
Lung cancer is far more treatable when detected early. Small, localised cancers can often be cured with surgery — sometimes even with a limited sublobar resection rather than removal of an entire lobe.
Waiting months or years to “see if a nodule grows” can delay diagnosis. While surveillance has a role in selected low-risk nodules, many nodules — particularly in patients with risk factors — should be biopsied promptly rather than simply observed.
Early diagnosis means:
- Greater likelihood of cure
- Less extensive surgery
- Faster reassurance if the nodule is benign
- Reduced psychological burden of “watching and waiting”
If we can safely biopsy small nodules early, we change outcomes.
The limitation of traditional bronchoscopy
Standard bronchoscopy has been used for decades to sample lung lesions. It works well for larger, centrally located abnormalities.
But many nodules detected on screening CT scans are:
- Small (often under 15 mm)
- Located in the outer third of the lung
- Close to the pleura
- In areas difficult to access with conventional scopes
Traditional bronchoscopy simply cannot reach many of these lesions with adequate precision.
For years, the alternative has been CT-guided percutaneous biopsy.
Robotic bronchoscopy vs CT-guided biopsy
CT-guided biopsy has an important role. But it has limitations — and risks.
Patient experience
- Robotic bronchoscopy: Performed under general anaesthesia. You’re asleep and comfortable.
- CT-guided biopsy: Performed while you are awake. Many patients find it distressing.
Risk of pneumothorax (collapsed lung)
- Robotic bronchoscopy: ~1%
- CT-guided biopsy: ~30%
A pneumothorax may require a chest drain and hospital admission. Avoiding this complication is significant.
Access to nodules
- Robotic bronchoscopy: Can access nodules anywhere in the lung, including bilateral lesions.
- CT-guided biopsy: Cannot safely reach up to 50% of nodules depending on location.
Robotic bronchoscopy allows navigation through the natural airway pathways, reaching peripheral nodules with remarkable precision.
For many patients, it should be considered before CT-guided biopsy.
What makes robotic bronchoscopy different?
Robotic-assisted bronchoscopy uses advanced navigation technology and a highly manoeuvrable catheter to reach small, difficult-to-access nodules.
It combines:
- High-resolution CT mapping
- 3D navigation
- Stable robotic control
- Real-time confirmation of tool position
The result is improved diagnostic yield for small peripheral nodules — particularly those that previously required either surveillance or higher-risk biopsy approaches.
First in Victoria
Dr Barton Jennings was one of the first two physicians in Victoria to perform robotic bronchoscopy.
Currently, Epworth Eastern is the only hospital in Victoria with this robotic bronchoscopy platform available.
Beyond diagnosis: placing fiducial markers for curative surgery
Robotic bronchoscopy does more than biopsy.
For small early cancers, we can place a fiducial marker coil at the time of biopsy. This tiny marker allows thoracic surgeons to accurately localise the lesion during minimally invasive robotic surgery.
Why does this matter?
Small nodules can be very difficult for surgeons to find during sublobar resection. A fiducial marker:
- Improves surgical precision
- Allows limited resection
- Preserves lung tissue
- Supports curative intent in early disease
Dr Jennings works closely with experienced thoracic surgeons to streamline this process — diagnosis and surgical planning working together from the outset.
Lung cancer screening is changing the landscape
With national screening now underway, more Australians aged 50–70 with a smoking history are eligible for low-dose CT scans.
Screening saves lives. But screening only works if abnormalities are managed efficiently and safely.
A structured approach includes:
- Rapid specialist review
- Risk assessment
- Multidisciplinary discussion
- Timely biopsy when indicated
- Coordinated surgical referral if required
This is exactly what we aim to provide.
Should lung nodules always be watched?
Not necessarily.
Small nodules in very low-risk individuals may be appropriate for surveillance. But many nodules particularly:
- ≥ 7 mm
- Show uptake on PET scan
- In smokers or ex-smokers
- Growing on interval imaging
These warrant biopsy rather than prolonged observation.
“Watch and wait” can feel passive and anxiety-provoking. For the right patient, early biopsy provides clarity.
A patient-centred approach
Hearing the words “lung nodule” is frightening.
Our goal is to replace uncertainty with a plan.
We provide:
- Rapid access appointments
- Clear explanation of options
- Multidisciplinary discussion when needed
- Advanced diagnostic technology
- Close collaboration with thoracic surgeons
- Ongoing support throughout the process
Early lung cancer can be cured.
But only if we diagnose it.
Considering robotic bronchoscopy?
If you’ve been told you have a lung nodule — particularly a small peripheral lesion — ask whether robotic bronchoscopy is appropriate before proceeding to CT-guided biopsy.
If you’re a GP or specialist referring a patient with an abnormal CT scan, we offer streamlined review and access to robotic biopsy when indicated.
Specialist care for better breathing — and for early, accurate answers when it matters most.
Book an appointment to speak with a respiratory specialist who listens.
Regular weekly bronchoscopy lists include:
- Robotic bronchoscopy – Epworth Eastern
- Bronchoscopy and EBUS – Epworth Richmond
- Bronchoscopy and EBUS – Cabrini Malvern
This consistent procedural volume is important. In advanced bronchoscopy, experience matters.

{kind=link}